

In the announcement of his new health care plan this week, Bernie Sanders claimed that the US spends more on health care than any other country, and he said it as if it were a bad thing.
The claim that the US spends more than anyone else can indeed be true, depending on what measurement you use. As a dollar amount for all spending, Americans are near the top. If you accept the World Health Organization’s, data — something that may or may not be advisable — then the spending breakdown looks like this:
 According to WHO, the US per capita spending is $8,467, followed by Norway at $6,106 and Luxembourg at $6,020.
Most of what puts the US above everyone else in this case is private spending. Rich countries in general spend more on health care since, even if one has access to taxpayer-financed health care, those with the means will often elect to pay for even more services (if the law allows). This isn’t just out-of-pocket, by the way. This is all spending in the private sector, so it includes the services already covered by a private insurance plan. Although health care is among the most regulated and subsidized industries in the country, most government transactions are technically “private”:
According to WHO, the US per capita spending is $8,467, followed by Norway at $6,106 and Luxembourg at $6,020.
Most of what puts the US above everyone else in this case is private spending. Rich countries in general spend more on health care since, even if one has access to taxpayer-financed health care, those with the means will often elect to pay for even more services (if the law allows). This isn’t just out-of-pocket, by the way. This is all spending in the private sector, so it includes the services already covered by a private insurance plan. Although health care is among the most regulated and subsidized industries in the country, most government transactions are technically “private”:
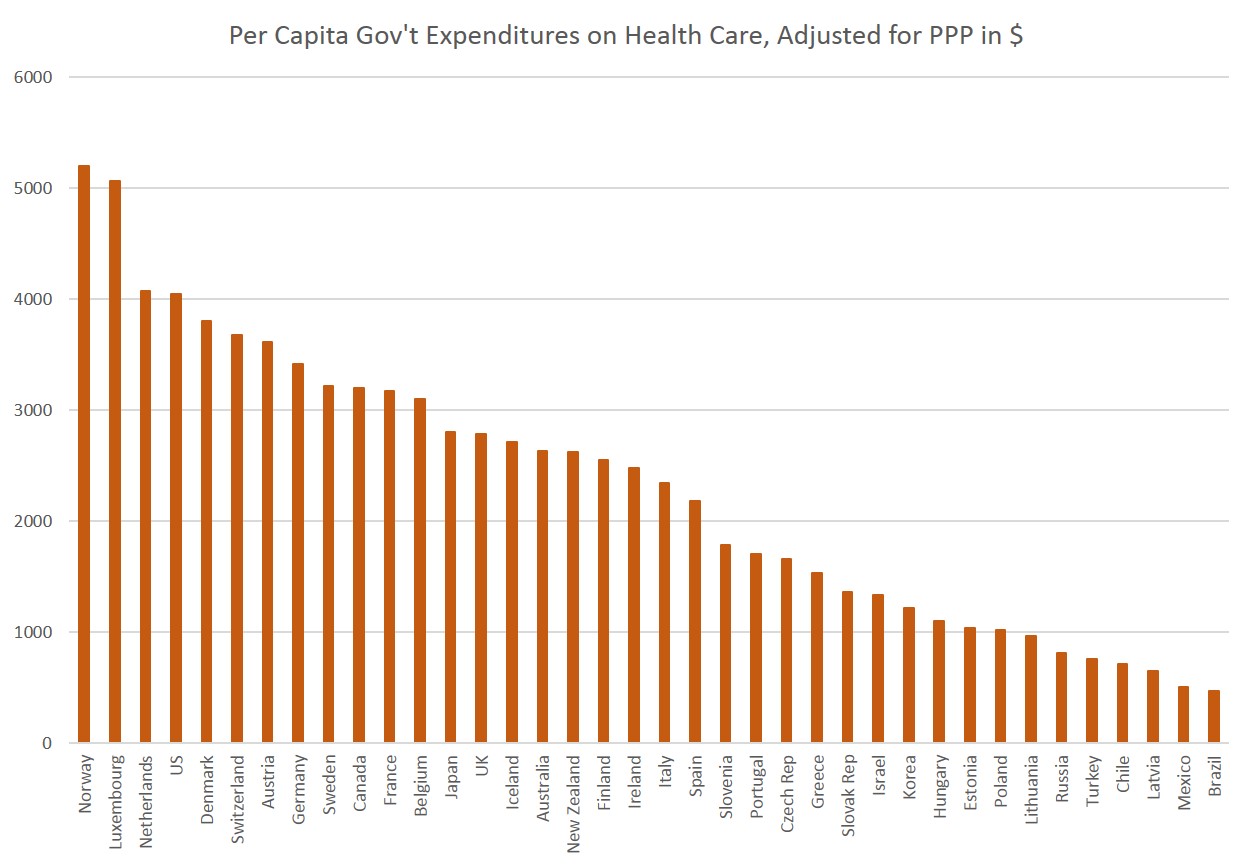
 Even after all that private spending, though, there’s still a whole lot of spending done by the government, and we find that in terms of government spending, the US is not an outlier at all, but is among the spendy-est of nations:
Even after all that private spending, though, there’s still a whole lot of spending done by the government, and we find that in terms of government spending, the US is not an outlier at all, but is among the spendy-est of nations:
 In this case, the US comes in at $4,047 behind Norway ($5,198), Luxembourg (5,061), and the Netherlands ($4,070), and is also quite comparable to Denmark ($3,801).
Wait, So Is Government Spending Now a Bad Thing?
Here’s where it gets silly, though. When we’re talking about government spending on social welfare programs, the US is often condemned for not spending enough. Americans are stingy, we’re told, and are so greedy, in fact, they refuse to tax themselves to pay for more welfare programs.
The truth, however, is that the US is among the biggest spenders on welfare in general, and on health care in particular.
By this measure put out by the OECD, in terms of direct government spending on welfare as a percentage of GDP, the US comes in at 19.2 percent, which means it spends more than Australia, Canada, and Iceland. Switzerland is nearly equal to the US at 19.4 percent, and Norway is at 22 percent. So, we’re apparently to believe that this alleged “free market” and social-Darwinist system in the US is defined by a 2 to 3 percent difference in spending when compared to Norway or the United Kingdom (21.7%).
And this doesn’t even take into account all the tax breaks that the US commonly uses to reduce the tax burden on low-income households. If those are taken into account, the OECD notes, then social expenditure in the US is even higher than Norway, Luxembourg, and many others.
Nor does the government neglect health spending as part of all that spending. The US, which spends 20.3 percent of government expenditures on health, ranks with Switzerland (21.1%), New Zealand (20.3%), and Japan (19.4%):
In this case, the US comes in at $4,047 behind Norway ($5,198), Luxembourg (5,061), and the Netherlands ($4,070), and is also quite comparable to Denmark ($3,801).
Wait, So Is Government Spending Now a Bad Thing?
Here’s where it gets silly, though. When we’re talking about government spending on social welfare programs, the US is often condemned for not spending enough. Americans are stingy, we’re told, and are so greedy, in fact, they refuse to tax themselves to pay for more welfare programs.
The truth, however, is that the US is among the biggest spenders on welfare in general, and on health care in particular.
By this measure put out by the OECD, in terms of direct government spending on welfare as a percentage of GDP, the US comes in at 19.2 percent, which means it spends more than Australia, Canada, and Iceland. Switzerland is nearly equal to the US at 19.4 percent, and Norway is at 22 percent. So, we’re apparently to believe that this alleged “free market” and social-Darwinist system in the US is defined by a 2 to 3 percent difference in spending when compared to Norway or the United Kingdom (21.7%).
And this doesn’t even take into account all the tax breaks that the US commonly uses to reduce the tax burden on low-income households. If those are taken into account, the OECD notes, then social expenditure in the US is even higher than Norway, Luxembourg, and many others.
Nor does the government neglect health spending as part of all that spending. The US, which spends 20.3 percent of government expenditures on health, ranks with Switzerland (21.1%), New Zealand (20.3%), and Japan (19.4%):
 So, if the US is spending nearly as much as, or even more than, the “generous” welfare states of northern Europe, why are we be constantly lectured about the need for more taxes and a larger role for government in everything?
Well, that’s when the advocates for even more taxpayer largesse change gears. “Don’t get me wrong,” they say. “We definitely need more taxes, and lots of them, but we need to spend those taxes differently.”
And that’s where the Bernie Sanders plan comes in. Sanders would like to overhaul the US health care system for the second time in five years, but this time, after instituting universal health care via a single-payer system, he’ll eventually make health care spending drop, and then we can cut taxes spend that tax money on something else.
How to Lower Costs: Revoke Choices for Patients
How will Sanders make the cost of health care go down? Well, that’s where things get murky, because the entire “plan” for doing this is about four pages long, and just based on the idea that administrative costs in the US are too high.
Writing in The New Yorker, James Surowiecki, who is hardly an advocate for laissez-faire, remains skeptical:
So, if the US is spending nearly as much as, or even more than, the “generous” welfare states of northern Europe, why are we be constantly lectured about the need for more taxes and a larger role for government in everything?
Well, that’s when the advocates for even more taxpayer largesse change gears. “Don’t get me wrong,” they say. “We definitely need more taxes, and lots of them, but we need to spend those taxes differently.”
And that’s where the Bernie Sanders plan comes in. Sanders would like to overhaul the US health care system for the second time in five years, but this time, after instituting universal health care via a single-payer system, he’ll eventually make health care spending drop, and then we can cut taxes spend that tax money on something else.
How to Lower Costs: Revoke Choices for Patients
How will Sanders make the cost of health care go down? Well, that’s where things get murky, because the entire “plan” for doing this is about four pages long, and just based on the idea that administrative costs in the US are too high.
Writing in The New Yorker, James Surowiecki, who is hardly an advocate for laissez-faire, remains skeptical:
 Below is the same scale imposed on North America.
It ranges from a high of 82 in British Columbia, Ontario, and Quebec, to 75 in West Virginia, Alabama, and Oklahoma. (Nearly all of Mexico is below 76 years, and Nunavut in Canada is at 71 years, although only 32,000 people live there.)
Most of the northern and Western US, however, has life expectancy levels at or above 80, putting is in the same category with Denmark, the UK, Belgium, and others.
Below is the same scale imposed on North America.
It ranges from a high of 82 in British Columbia, Ontario, and Quebec, to 75 in West Virginia, Alabama, and Oklahoma. (Nearly all of Mexico is below 76 years, and Nunavut in Canada is at 71 years, although only 32,000 people live there.)
Most of the northern and Western US, however, has life expectancy levels at or above 80, putting is in the same category with Denmark, the UK, Belgium, and others.
 Moreover, what we find is that, while all the US health care law is dominated by federal law, the differences in state life expectancy statistics can range by several years depending on regional factors. In other words, health care law in the US is nationwide, but health care outcomes vary significantly by region.
Logically, this would lead us to believe that health care outcomes depend on something more than mere public policy, including obesity rates, foreign born populations, and ethnic makeup. (See here for more.)
These issues can have profound effects on health outcomes, and although its been recently implied in the context of migrants that Europe is very ethnically diverse, the reality is that European countries are far more ethnically uniform, far more “white” than the US, and definitely less fat.
Indeed, if the US had an ethnic mix like Canada, where the largest non-white group is Asians (who have higher life expectancy than whites), and where the percentage of immigrants is higher than it is in the US, the life expectancy of the US would immediately increase significantly. (In North America, immigrants are healthier than natives.) Like Europeans, Canadians are also less obese than Americans.
Conclusions
None of what I say here should be regarded as an endorsement of the American health care system which today is largely a hodgepodge of government regulations and historical accidents that led to the creation of a system driven by huge insurance conglomerates in a response to federal public policy after World War II. It’s a system that encourages more private spending on health care, by the way.
There is, of course, nothing “free-market” or laissez faire about American health care.
However, we should also be realistic about the effects of the suggested alternatives, which seek primarily to replace a highly regulated system with a totally centrally-planned one. Both are very sub-optimal, and a shift from the current system to a new system will bring both costs and benefits for different groups.
But, this idea that a move to a European-style system of health care will slash costs is based on nothing more than pure speculation, which is why no details are provided. In the meantime, taxpayers will be expected to pay far more in taxes. And in the midst of it all, there’s no reason to believe that outcomes will be changed significantly in light of the realities of lifestyle, demographics, and geography.
Moreover, what we find is that, while all the US health care law is dominated by federal law, the differences in state life expectancy statistics can range by several years depending on regional factors. In other words, health care law in the US is nationwide, but health care outcomes vary significantly by region.
Logically, this would lead us to believe that health care outcomes depend on something more than mere public policy, including obesity rates, foreign born populations, and ethnic makeup. (See here for more.)
These issues can have profound effects on health outcomes, and although its been recently implied in the context of migrants that Europe is very ethnically diverse, the reality is that European countries are far more ethnically uniform, far more “white” than the US, and definitely less fat.
Indeed, if the US had an ethnic mix like Canada, where the largest non-white group is Asians (who have higher life expectancy than whites), and where the percentage of immigrants is higher than it is in the US, the life expectancy of the US would immediately increase significantly. (In North America, immigrants are healthier than natives.) Like Europeans, Canadians are also less obese than Americans.
Conclusions
None of what I say here should be regarded as an endorsement of the American health care system which today is largely a hodgepodge of government regulations and historical accidents that led to the creation of a system driven by huge insurance conglomerates in a response to federal public policy after World War II. It’s a system that encourages more private spending on health care, by the way.
There is, of course, nothing “free-market” or laissez faire about American health care.
However, we should also be realistic about the effects of the suggested alternatives, which seek primarily to replace a highly regulated system with a totally centrally-planned one. Both are very sub-optimal, and a shift from the current system to a new system will bring both costs and benefits for different groups.
But, this idea that a move to a European-style system of health care will slash costs is based on nothing more than pure speculation, which is why no details are provided. In the meantime, taxpayers will be expected to pay far more in taxes. And in the midst of it all, there’s no reason to believe that outcomes will be changed significantly in light of the realities of lifestyle, demographics, and geography.
 According to WHO, the US per capita spending is $8,467, followed by Norway at $6,106 and Luxembourg at $6,020.
Most of what puts the US above everyone else in this case is private spending. Rich countries in general spend more on health care since, even if one has access to taxpayer-financed health care, those with the means will often elect to pay for even more services (if the law allows). This isn’t just out-of-pocket, by the way. This is all spending in the private sector, so it includes the services already covered by a private insurance plan. Although health care is among the most regulated and subsidized industries in the country, most government transactions are technically “private”:
According to WHO, the US per capita spending is $8,467, followed by Norway at $6,106 and Luxembourg at $6,020.
Most of what puts the US above everyone else in this case is private spending. Rich countries in general spend more on health care since, even if one has access to taxpayer-financed health care, those with the means will often elect to pay for even more services (if the law allows). This isn’t just out-of-pocket, by the way. This is all spending in the private sector, so it includes the services already covered by a private insurance plan. Although health care is among the most regulated and subsidized industries in the country, most government transactions are technically “private”:
 Even after all that private spending, though, there’s still a whole lot of spending done by the government, and we find that in terms of government spending, the US is not an outlier at all, but is among the spendy-est of nations:
Even after all that private spending, though, there’s still a whole lot of spending done by the government, and we find that in terms of government spending, the US is not an outlier at all, but is among the spendy-est of nations:
 In this case, the US comes in at $4,047 behind Norway ($5,198), Luxembourg (5,061), and the Netherlands ($4,070), and is also quite comparable to Denmark ($3,801).
Wait, So Is Government Spending Now a Bad Thing?
Here’s where it gets silly, though. When we’re talking about government spending on social welfare programs, the US is often condemned for not spending enough. Americans are stingy, we’re told, and are so greedy, in fact, they refuse to tax themselves to pay for more welfare programs.
The truth, however, is that the US is among the biggest spenders on welfare in general, and on health care in particular.
By this measure put out by the OECD, in terms of direct government spending on welfare as a percentage of GDP, the US comes in at 19.2 percent, which means it spends more than Australia, Canada, and Iceland. Switzerland is nearly equal to the US at 19.4 percent, and Norway is at 22 percent. So, we’re apparently to believe that this alleged “free market” and social-Darwinist system in the US is defined by a 2 to 3 percent difference in spending when compared to Norway or the United Kingdom (21.7%).
And this doesn’t even take into account all the tax breaks that the US commonly uses to reduce the tax burden on low-income households. If those are taken into account, the OECD notes, then social expenditure in the US is even higher than Norway, Luxembourg, and many others.
Nor does the government neglect health spending as part of all that spending. The US, which spends 20.3 percent of government expenditures on health, ranks with Switzerland (21.1%), New Zealand (20.3%), and Japan (19.4%):
In this case, the US comes in at $4,047 behind Norway ($5,198), Luxembourg (5,061), and the Netherlands ($4,070), and is also quite comparable to Denmark ($3,801).
Wait, So Is Government Spending Now a Bad Thing?
Here’s where it gets silly, though. When we’re talking about government spending on social welfare programs, the US is often condemned for not spending enough. Americans are stingy, we’re told, and are so greedy, in fact, they refuse to tax themselves to pay for more welfare programs.
The truth, however, is that the US is among the biggest spenders on welfare in general, and on health care in particular.
By this measure put out by the OECD, in terms of direct government spending on welfare as a percentage of GDP, the US comes in at 19.2 percent, which means it spends more than Australia, Canada, and Iceland. Switzerland is nearly equal to the US at 19.4 percent, and Norway is at 22 percent. So, we’re apparently to believe that this alleged “free market” and social-Darwinist system in the US is defined by a 2 to 3 percent difference in spending when compared to Norway or the United Kingdom (21.7%).
And this doesn’t even take into account all the tax breaks that the US commonly uses to reduce the tax burden on low-income households. If those are taken into account, the OECD notes, then social expenditure in the US is even higher than Norway, Luxembourg, and many others.
Nor does the government neglect health spending as part of all that spending. The US, which spends 20.3 percent of government expenditures on health, ranks with Switzerland (21.1%), New Zealand (20.3%), and Japan (19.4%):
 So, if the US is spending nearly as much as, or even more than, the “generous” welfare states of northern Europe, why are we be constantly lectured about the need for more taxes and a larger role for government in everything?
Well, that’s when the advocates for even more taxpayer largesse change gears. “Don’t get me wrong,” they say. “We definitely need more taxes, and lots of them, but we need to spend those taxes differently.”
And that’s where the Bernie Sanders plan comes in. Sanders would like to overhaul the US health care system for the second time in five years, but this time, after instituting universal health care via a single-payer system, he’ll eventually make health care spending drop, and then we can cut taxes spend that tax money on something else.
How to Lower Costs: Revoke Choices for Patients
How will Sanders make the cost of health care go down? Well, that’s where things get murky, because the entire “plan” for doing this is about four pages long, and just based on the idea that administrative costs in the US are too high.
Writing in The New Yorker, James Surowiecki, who is hardly an advocate for laissez-faire, remains skeptical:
So, if the US is spending nearly as much as, or even more than, the “generous” welfare states of northern Europe, why are we be constantly lectured about the need for more taxes and a larger role for government in everything?
Well, that’s when the advocates for even more taxpayer largesse change gears. “Don’t get me wrong,” they say. “We definitely need more taxes, and lots of them, but we need to spend those taxes differently.”
And that’s where the Bernie Sanders plan comes in. Sanders would like to overhaul the US health care system for the second time in five years, but this time, after instituting universal health care via a single-payer system, he’ll eventually make health care spending drop, and then we can cut taxes spend that tax money on something else.
How to Lower Costs: Revoke Choices for Patients
How will Sanders make the cost of health care go down? Well, that’s where things get murky, because the entire “plan” for doing this is about four pages long, and just based on the idea that administrative costs in the US are too high.
Writing in The New Yorker, James Surowiecki, who is hardly an advocate for laissez-faire, remains skeptical:
The answer in the document is vague: “Reforming our health care system, simplifying our payment structure and incentivizing new ways to make sure patients are actually getting better health care will generate massive savings.” The general idea seems to be that moving to the single-payer model will lead to a huge drop in administrative costs, and will also allow the government to use its leverage to drive down the prices of drugs and medical devices. According toan analysis that the campaign released by Gerald Friedman, a professor of economics at the University of Massachusetts at Amherst, costs in the new system would also rise much more slowly than they do today. Sanders claims that, all told, his plan will save ten trillion dollars across ten years.Neither the plan nor Friedman explains where those ten trillion dollars would come from.Surowiecki concludes:
The truth is that if you want to save a trillion dollars a year in health-care spending, you can’t do it solely by cutting administrative costs and drug prices.High health care costs in the US are a byproduct of US consumer choices and a variety of factors far beyond the fact that administrative costs are high. Victor Fuchs writes in The Atlantic:
Why does the United States spend so much more? The biggest reason is that U.S. healthcare delivers a more expensive mix of services. For example, a much larger proportion of physician visits in the U.S. are to specialists who get higher fees and usually order more high-tech diagnostic and therapeutic procedures than primary care physicians.
Compared with the average OECD country, the U.S. delivers (population adjusted) almost three times as many mammograms, two-and-a-half times the number of MRI scans, and 31 percent more C-sections. Also, the U.S. has more stand-by equipment, for example, 1.66 MRI machines per 6,000 annual scans vs. 1.06 machines. The extra machines provide easier access for Americans, but add to cost.
Similarly, occupancy rates in U.S. acute care hospitals are much lower than in OECD countries, reducing the likelihood of delays in admissions, but building that extra capacity adds to cost. Aggressive treatment of very sick elderly also makes the mix expensive. In the U.S. many elderly patients are treated in intensive care units (ICUs), but in other countries they would receive only palliative care. More amenities such as privacy and space in hospitals and more attractive clinics also add to U.S. costs.
While the U.S. mix of services is disproportionately tilted toward more expensive interventions, the other OECD countries emphasize a “plain vanilla” mix. Compared with the U.S., the average OECD country has 30 percent more physician visits and more than 30 percent more hospital days per capita.One can agree or disagree from a medical perspective as to whether or not all those C-sections and tests are a good thing, but the fact of the matter is that Americans seem to have no problem with taking advantage of all these “extra” health services. Old people are free to refuse intensive efforts to save their lives, and opt for the European model of letting very-ill old people die sooner rather than later to save money. But many choose procedures designed to prolong their lives instead of merely ease their pain. These are choices that real people make, and the only way to truly cut the cost of health care in such a system is to diminish the ability of people to make these choices. Rather than leave these decisions up to the individuals, who may opt for more expensive options, these choices would instead have to be made by government administrators who are tasked with keeping costs under control, and who enjoy a monopoly on the provision of services. Now, even if one has no particular problem with government control of the health care system, anyone who’s honest about any political decision knows that there are both winners and losers, and upsides and downsides. There are upsides to single-payer type health care if you’re low-income and all you need is some antibiotics or a hernia surgery. However, if your problem involves difficult diagnostic problems, you may need to opt for the more “expensive” health care system, even if you’re low income. To suggest, however, that a move to a single-payer system is all “upside” as Sanders is doing, is profoundly dishonest. But What About Outcomes? Having been robbed of the idea that the US welfare state is unusually stingy, the advocates for more welfare must then fall back on the idea that the outcomes are worse, so, therefore, the US taxpayers must both spend more and spend differently. The problem is that it is not at all obvious that the outcomes would be significantly different after some additional tinkering with the system. After all, the divergence between US outcomes and the outcomes in the supposedly superior systems of western Europe can be quite small. Here’s a map of life expectancy at birth for Europe, using OECD data. It ranges from the mid-70s in Russia and Eastern Europe, to 83 in Iceland and Switzerland. Government-provided health care is the norm throughout Europe, including Eastern Europe:
 Below is the same scale imposed on North America.
It ranges from a high of 82 in British Columbia, Ontario, and Quebec, to 75 in West Virginia, Alabama, and Oklahoma. (Nearly all of Mexico is below 76 years, and Nunavut in Canada is at 71 years, although only 32,000 people live there.)
Most of the northern and Western US, however, has life expectancy levels at or above 80, putting is in the same category with Denmark, the UK, Belgium, and others.
Below is the same scale imposed on North America.
It ranges from a high of 82 in British Columbia, Ontario, and Quebec, to 75 in West Virginia, Alabama, and Oklahoma. (Nearly all of Mexico is below 76 years, and Nunavut in Canada is at 71 years, although only 32,000 people live there.)
Most of the northern and Western US, however, has life expectancy levels at or above 80, putting is in the same category with Denmark, the UK, Belgium, and others.
 Moreover, what we find is that, while all the US health care law is dominated by federal law, the differences in state life expectancy statistics can range by several years depending on regional factors. In other words, health care law in the US is nationwide, but health care outcomes vary significantly by region.
Logically, this would lead us to believe that health care outcomes depend on something more than mere public policy, including obesity rates, foreign born populations, and ethnic makeup. (See here for more.)
These issues can have profound effects on health outcomes, and although its been recently implied in the context of migrants that Europe is very ethnically diverse, the reality is that European countries are far more ethnically uniform, far more “white” than the US, and definitely less fat.
Indeed, if the US had an ethnic mix like Canada, where the largest non-white group is Asians (who have higher life expectancy than whites), and where the percentage of immigrants is higher than it is in the US, the life expectancy of the US would immediately increase significantly. (In North America, immigrants are healthier than natives.) Like Europeans, Canadians are also less obese than Americans.
Conclusions
None of what I say here should be regarded as an endorsement of the American health care system which today is largely a hodgepodge of government regulations and historical accidents that led to the creation of a system driven by huge insurance conglomerates in a response to federal public policy after World War II. It’s a system that encourages more private spending on health care, by the way.
There is, of course, nothing “free-market” or laissez faire about American health care.
However, we should also be realistic about the effects of the suggested alternatives, which seek primarily to replace a highly regulated system with a totally centrally-planned one. Both are very sub-optimal, and a shift from the current system to a new system will bring both costs and benefits for different groups.
But, this idea that a move to a European-style system of health care will slash costs is based on nothing more than pure speculation, which is why no details are provided. In the meantime, taxpayers will be expected to pay far more in taxes. And in the midst of it all, there’s no reason to believe that outcomes will be changed significantly in light of the realities of lifestyle, demographics, and geography.
Moreover, what we find is that, while all the US health care law is dominated by federal law, the differences in state life expectancy statistics can range by several years depending on regional factors. In other words, health care law in the US is nationwide, but health care outcomes vary significantly by region.
Logically, this would lead us to believe that health care outcomes depend on something more than mere public policy, including obesity rates, foreign born populations, and ethnic makeup. (See here for more.)
These issues can have profound effects on health outcomes, and although its been recently implied in the context of migrants that Europe is very ethnically diverse, the reality is that European countries are far more ethnically uniform, far more “white” than the US, and definitely less fat.
Indeed, if the US had an ethnic mix like Canada, where the largest non-white group is Asians (who have higher life expectancy than whites), and where the percentage of immigrants is higher than it is in the US, the life expectancy of the US would immediately increase significantly. (In North America, immigrants are healthier than natives.) Like Europeans, Canadians are also less obese than Americans.
Conclusions
None of what I say here should be regarded as an endorsement of the American health care system which today is largely a hodgepodge of government regulations and historical accidents that led to the creation of a system driven by huge insurance conglomerates in a response to federal public policy after World War II. It’s a system that encourages more private spending on health care, by the way.
There is, of course, nothing “free-market” or laissez faire about American health care.
However, we should also be realistic about the effects of the suggested alternatives, which seek primarily to replace a highly regulated system with a totally centrally-planned one. Both are very sub-optimal, and a shift from the current system to a new system will bring both costs and benefits for different groups.
But, this idea that a move to a European-style system of health care will slash costs is based on nothing more than pure speculation, which is why no details are provided. In the meantime, taxpayers will be expected to pay far more in taxes. And in the midst of it all, there’s no reason to believe that outcomes will be changed significantly in light of the realities of lifestyle, demographics, and geography. 
